Learn more about pain.

Pain is a universal human experience, affecting millions of patients in the US each year and is caused by many things, including injury, surgery, illness, trauma, and burns. Pain sends more people to healthcare providers than anything else.1 It significantly reduces quality of life, impacting our daily activities, productivity, and mental well-being.
Why do we feel pain?
The experience of pain begins often with an injury or wound that initiates a message traveling from the affected area along the spinal cord up toward the brain regions that process and interpret the sensation.2 The brain then launches a descending message that projects back down the spinal cord releasing endogenous opioids, our body’s natural painkillers, that bind to opioid receptors.2 This action helps to modulate or inhibit the incoming noxious information, effectively lessening the perception of pain.2
The challenges and tradeoffs in treating serious pain
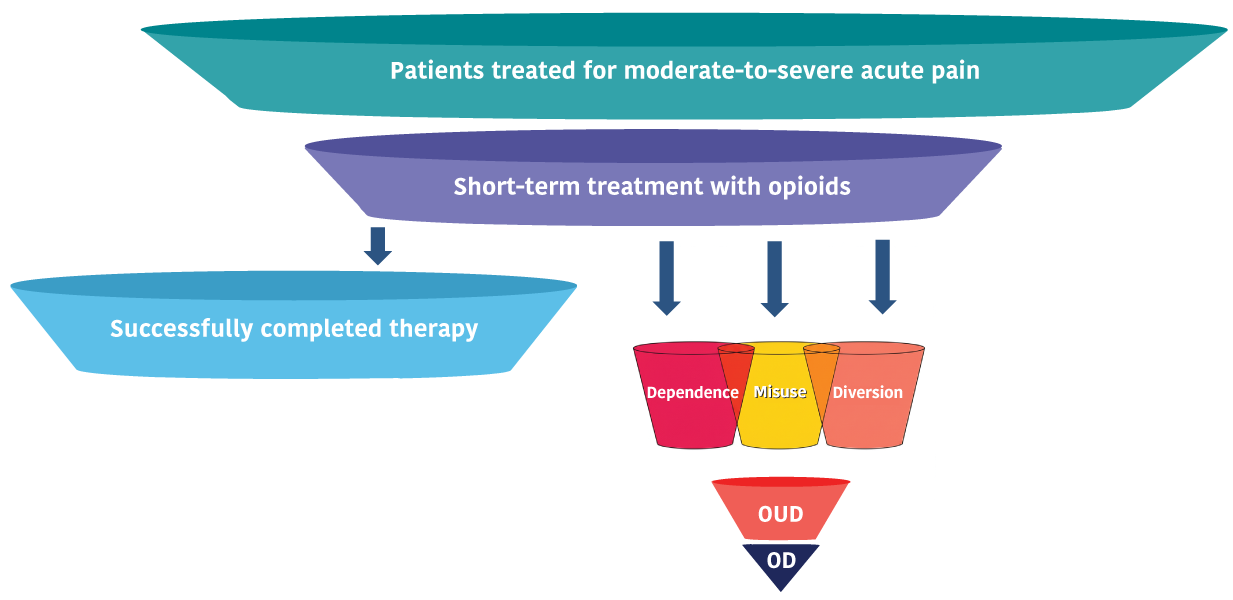
Moderate-to-severe acute pain associated with surgery and medical procedures can often only be effectively treated with preferential MOP agonist analgesics (such as oxycodone, hydrocodone, hydromorphone, etc.) especially following joint replacements, orthopedic and invasive procedures, major traumas, and burns.2
Even short-term use of conventional opioids (preferential MOP agonists) may carry significant risks:
- Addiction risk3
- Dependence in 11-13% of patients within just 5 days of use4,5
- Misuse and diversion because of their euphoria-inducing effects6,7
“Acute pain ignored, chronic pain endured”
While conventional opioids remain the most effective option for treating moderate to severe acute pain, their utilization is limited due to serious side effects. Data have shown that in the aftermath of the opioid crisis and ongoing concerns from physicians and patients about potential addiction or adverse effects, some acute pain is going undertreated or untreated, creating a substantial gap in pain management and leaving the door open to long-term consequences, including chronic pain.8-11
Risk of Chronic post-surgical pain (CPSP)
- Hip arthroplasty 27% risk of CPSP12,13
- Knee arthroplasty between 13%-44%12,13
The less visible impact of pain
Concerns about dependence, misuse, and opioid use disorder have influenced the prescribing practices of physicians and reduced the acceptance of conventional opioids by patients, leading to the potential undertreatment of acute pain.11
- The undertreatment of acute pain carries its own consequences, including the potential shift from acute to chronic pain and poorer long-term outcomes.11
- The risk of developing chronic pain is two to three times greater when severe acute pain is treated ineffectively in the first days following surgery or injury.11
Both the use of conventional opioids and the withholding of them require careful consideration when determining how to treat pain effectively and minimize unintended adverse effects. Read more about how the opioid crisis continues to influence the treatment of pain in “The burden of acute pain in the U.S. in the wake of the opioid crisis” published in Frontiers in Pain Research, 2025.
How can we provide the most effective pain relief without exposing patients to possible risk of life-threatening side effects?
Today, there is more need than ever for new tools to address acute pain (sudden, sharp, or intense pain), as we see the annual number of surgeries increase, the population ages, and metabolic disease rates climb.
Adneuris Therapeutics is developing cebranopadol, which has the potential to deliver potent pain relief with a strong safety profile. Cebranopadol is a dual-NMR agonist, which leverages the modulatory role of the NOP receptor on the activation of the MOP, which reduces the adverse effects associated with conventional opioids.
“Studies have shown that the experience of euphoria plays a significant role in driving the desire to continue using opioids beyond the point of medical need.”*
Physical dependence on opioids can occur in as few as 5 days’ use.*
Based on a thorough review of data from preclinical studies, the National Institute on Drug Abuse, part of the National Institutes of Health, has awarded Adneuris Therapeutics up to $16.6 million to further evaluate cebranopadol’s potential as a treatment for OUD. Under the grant, we will collaborate with renowned addiction experts to complete preclinical through Phase 2 studies.**
*Hackworth JC, Schneider JE, Do Valle M, et al. The burden of acute pain in the U.S. in the wake of the opioid crisis. Front Pain Res. Hackworth JC, Schneider JE, Do Valle M, et al. The burden of acute pain in the U.S. in the wake of the opioid crisis. Front Pain Res. 2025;6:1642035.
**Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number UG3DA059285. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References:
- Nahin RL, Sayer B, Stussman BJ, Feinberg TM. Eighteen-year trends in the prevalence of, and health care use for, noncancer pain in the United States: Data from the medical expenditure panel survey. J Pain. 2019;20(7):796-809.
- Yam MF, Loh YC, Tan CS, et al. General pathways of pain sensation and the major neurotransmitters involved in pain regulation. Int J Mol Sci. 2018;19(8):2164.
- Han B, Jones CM, Einstein EB, Dowell D, Compton WM. Prescription opioid use disorder among adults reporting prescription opioid use with or without misuse in the United States. J Clin Psychiatry. 2024;85(3).
- Fishbain DA, Cole B, Lewis J, Rosomoff HL, Rosomoff RS. What percentage of chronic nonmalignant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review. Pain Med. 2008;9(4):444–459.
- Meisel ZF, Lupulescu-Mann N, Charlesworth CJ, Kim H, Sun BC. Conversion to persistent or high-risk opioid use after a new prescription from the emergency department: Evidence from Washington Medicaid beneficiaries. AnnEmerg Med. 2019;74(5):611–621.
- Wightman R, Perrone J, Portelli I, Nelson L. Likeability and abuse liability of commonly prescribed opioids. J Med Toxicol. 2012 Dec;8(4):335-40.
- Abril Ochoa L, Naeem F, White DJ, Bijur PE, Friedman BW. Opioid-induced euphoria among emergency department patients with acute severe pain: An analysis of data from a randomized trial. AcadEmergMed. 2020;27(11):1100-1105.
- Fregoso G, Wang A, Tseng K, Wang J. Transition from acute to chronic pain: Evaluating risk for chronic postsurgical pain. Pain Physician. 2019;22(5):479-88.
- Pak DJ, Yong RJ, Kaye AD, Urman RD. Chronification of pain: Mechanisms, current understanding, and clinical implications. Curr Pain Headache Rep. 2018;22(2):9.
- Pozek JP, Beausang D, Baratta JL, Viscusi ER. The acute to chronic pain transition: Can chronic pain be prevented? Med Clin North Am. 2016;100(1):17-30.
- Hackworth JC, Schneider JE, Do Valle M, et al. The burden of acute pain in the U.S. in the wake of the opioid crisis. Front Pain Res. 2025;6:1642035.
- Bruce J, Quinlan J. Chronic post surgical pain. Rev Pain. 2011;5(3):23-9.
- Schug SA, Bruce J. Risk stratification for the development of chronic postsurgical pain. Pain Rep. 2017;2(6):e627.

